
The age of cancer: February 2021 saw the release of the ‘Europe’s Beating Cancer Plan’ by the European Commission. With cancer poised to become the EU’s leading cause of death by 2035 and with treatment and survival rates varying dramatically between Member States and societal groups, how should the EU ensure equal access to cancer treatment?
Chaired by Raphael Gross-Chartuni (NL)
‘Declare the past, diagnose the present, and foretell the future .’
– Hippocrates, Ancient Greek physician
The Topic at a Glance
Cancer is older than humanity itself. Despite countless advancements in oncology and biopharmaceutics, cancer remains an inevitability.
In 2020, over 2.7 million people in the EU were diagnosed with cancer and 1.3 million lives were taken by it. The European economy is impacted as well, with an annual sum of over EUR 100 billion lost due to cancer. Moreover, some reports estimate the cancer incidence will increase by as much as 24%, making it the primary cause of death in the EU by 2035.
In response to this prospect, the EU has set out a new goal in which cancer is defeated. On 21 of February 2021, the EU announced the Europe’s Beating Cancer Plan. This entails a budget of EUR 4 billion, allocated towards the plan’s four pillars: prevention, early detection, diagnosis and treatment, and the well-being of both patients and survivors.
Combating cancer, a multifaceted and complex disease, requires tremendous efforts and a wide range of solutions. These range from information campaigns and taxation schemes for tobacco and alcohol consumption to complex data networks to centralise cancer research and treatment. However, when looking at cancer diagnosis and survival rates, there are major discrepancies between the Member States. Similar differences can be seen between age groups, socioeconomic, and even racial demographics. This inaccessibility of treatments based on income or geographical factors poses a threat to the lives of many European citizens. Furthermore, inequality is not only observed with the diagnosis and treatment of cancer itself, as many patients are met with workplace discrimination. The war on cancer is fought on all fronts and requires sufficient legislation to turn each battle into a victory. This not only entails treatment for individual patients, but efforts from Europe united as one.
Keywords
- Cancer is a disease in which unregulated cell-growth causes tumours. The subsequent complications are deadly if left untreated.
- Substances like formaldehyde and benzene, which cause cancer, are called carcinogens.
- Therapeutics are medicines used for treatment.
- Cancer incidence is the relative occurrence of cancer in a demographic. Incidence rates depend on the amount of diagnosed cancer per predetermined population.
- Cancer mortality refers to death attributed to cancer. Mortality rates depend on the amount of mortality per predetermined population.
Key Stakeholders
As cancer affects us all, everyone from both the individual and the societal level is a stakeholder. Yet, there remain prominent groups and entities which play a significant role.
The European Commission is responsible for the execution of the Europe’s Beating Cancer Plan. The Commission is the executive organ of the EU which proposes and enforces EU legislation.
This plan receives funding from primarily two sources: EU4Health and Horizon Europe. The former is led by the European Health and Digital Executive Agency (HaDEA), the latter directly by the Commission. Horizon Europe is the primary funding programme for innovation and research in the EU, allocating a portion of its EUR 95,5 billion budget to cancer research as well.
Additionally, the Commission set up a Knowledge Centre on Cancer in 2021. It will play an important role in the fight against cancer as it manages large databases containing patient and cancer data and develops both guidelines and quality assurance schemes on a European level.
Representing the (bio)pharmaceutical industry in the EU, the European Federation of Pharmaceutical Industries and Associations (EFPIA) communicates with EU bodies on pharmaceutical matters. The EFPIA contains a board with representatives from European pharmaceutical companies, as well as a delegation with members from international corporations, primarily non-EU. The Commission has expressed the need for better communication and integration with the pharmaceutical industry for the development and distribution of new therapeutics, meaning that the EFPIA will play a significantly bigger role in the future.
This role is in close relation to the European Medicines Agency (EMA), which approves novel therapies and monitors currently used drugs on the EU-level.
Considering the rise in the exchange of patient data, the European Data Protection Board (EDPB) enforces the General Data Protection Regulation (GDPR), which harmonises the gathering and exchange of data from European citizens by corporations and governments. The EDPB advises the Commission on cases of data protection and resolves legal disputes between national supervisory authorities.
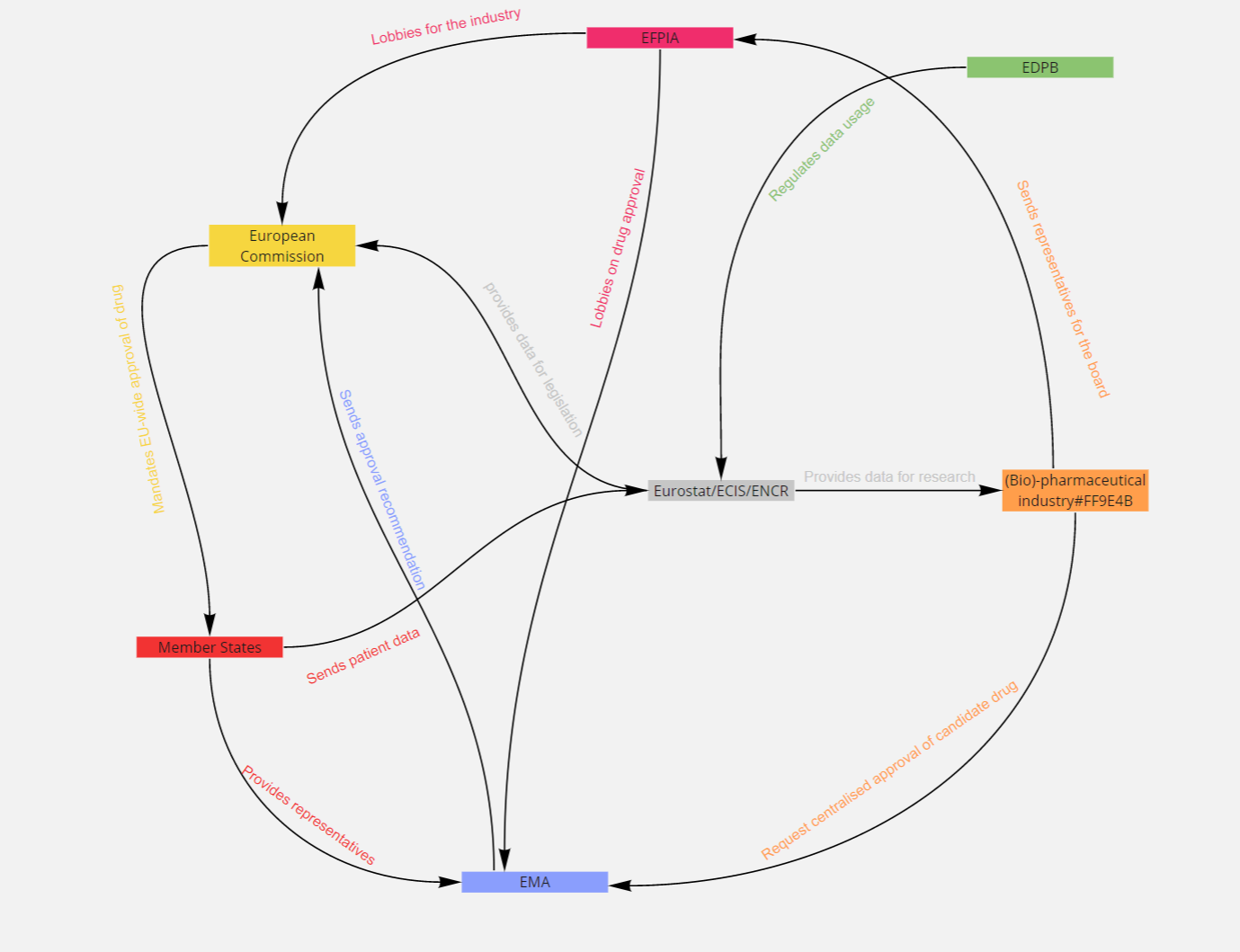
Figure 1: The Key Stakeholders of the Topic.
Key Conflicts
A remedy to disharmony
While the EU pushes for solidarity in the war against cancer, the battle is not fought equally on each front. Significant discrepancies are found in both cancer mortality and incidence across the Member States. Generally speaking, the number of people with a predisposition for breast cancer who are tested varies from 6% to 90% among Member States, and the subsequent survival rate by 20%. Statistical analyses show that in all Eastern European Countries, aside from Cyprus, the mortality rates are significantly higher than in Western Europe when compared to the same incidence rates.
One reason for this seems to be that Western European countries have higher expenditures towards healthcare than Eastern Europe, which results in more available treatment options for patients and more early screenings.
On the other hand, the cancer incidence in Eastern Europe is generally lower than in Western Europe, despite the higher mortality rates. What can the EU do to minimise the inconsistent mortality gaps between the Member States while respecting their autonomy? What can the EU further do to close the cancer data gaps and minimal screening across certain Member States?
A prayer to Panacea
A major issue is the (in)availability of cancer therapies. Reports have shown that EMA approval of medication does not equate to immediate access across Europe. There are major differences between drug approval rates between the Member States. For instance, patients in Germany have full access to all drugs approved by the EMA between 2006-2016 against several types of cancer, while Scotland only allows access to less than 40% of those same drugs.
According to Lung Cancer Europe (LuCE), Eastern European countries often do not reimburse treatments, while Western European countries usually offer full subsidies. In the event where a patient can afford such expensive therapies, treatment is not always guaranteed due to national legislation. For instance, patients in Poland have minimal access as treatment from self-paid drugs is not covered by the state either, which prompts hospitals to deny such requests. This increases the need to go abroad for therapy, thereby adding additional costs and restraints like language and cultural barriers.
As drug responses are based on countless factors, including a patient’s individual biology and type(s) of cancer, a wide range of medications must be available to maximise the odds of survival. What role can the EU play to further diminish the dire dissonance in drug availability between the Member States? What can the EU do for those whose treatment is denied?
To cause or not to cause
Controlling environmental factors is a necessary tool to prevent cancer caused from airborne matter. Initiatives such as smoke-free policies in Ireland and Scotland have improved indoor air quality by as much as 85%, with major effects on the occurrence of oral, throat, and lung cancer. In Eastern Europe, however, only minimal efforts have been taken to improve air quality and reduce tobacco consumption and exposure to airborne or particulate carcinogens. This has led to air pollution levels being far above the guidelines from the World Health Organization (WHO). In 2016, 87,4 per 100.000 people died from lung cancer in Hungary, while in Sweden that rate was only 35,3.
However, not all carcinogenic exposure is derived from tobacco consumption or air pollution. Occupational exposure is a major problem in the EU. Many jobs are linked to several types of cancer. For instance, pesticides such as glyphosate are used in the agricultural sector in Germany and the Netherlands, despite being controversial due to potential cancer risk. While the European Food Safety Authority (EFSA) approved its use, a scientific analysis declared that 34 out of the 53 industry-backed studies cited by the EFSA were unreliable.
In other parts of Europe, the economy relies on different industries and thus presents its own unique set of workplace carcinogens. What can the EU do to tackle occupational carcinogenicity as a whole, while tailoring its approaches to individual Member States? What measures can the EU take to avoid further discordance between legislators and experts on carcinogenic substances?
{kind=link}
Aesculapian bias
While cancer does not discriminate, the people who suffer from it are discriminated against. Despite access to medicines being a fundamental aspect of human rights, the availability is heavily dependent on economic factors. Many novel therapeutics are not fully covered by insurance and require additional or full payment.
But not all costs are related to the treatment itself. Much of these out-of-pocket expenses are directed towards caregivers, transporting patients, and drugs such as painkillers.
This brings up the point of workplace discrimination. Many patients and survivors receive unfair lay-offs or are denied promotions, as is common with most chronic or long-term diseases. Furthermore, the prospect of the Europe’s Beating Cancer plan revolves around generating and distributing large amounts of clinical and genetic patient data. This brings the danger of discrimination of patients applying for contracts such as mortgages, health insurance, or loans. What steps can the EU take to nullify the socioeconomic and geographical burdens of patients? What can the EU do to prevent workplace discrimination and future financial discrimination from creditors?
Measures in Place
Prior to the new Europe’s Beating Cancer Plan, many systems and schemes have been put in place in the fight against cancer. As cancer diagnosis and treatment must be tested empirically, the need for data gathering is big. Several organisations monitor cancer cases across Europe, the most prominent being Eurostat, the European Cancer Information System (ECIS), and the European Network of Cancer Registries (ENCR). They collect and make data available for research. In 2017, a five-year joint effort between 30 countries, the European Environment Agency (EEA) and the Commission commenced under the Horizon Europe programme. The goal of HBM4EU was to monitor European citizens’ exposure to cancer-causing chemicals.
Additionally, the EU has made headway in reducing tobacco usage. In 2001, the EU adopted a directive regulating the manufacturing, presentation, and sale of tobacco products in the EU. A significant rework was established in 2014, aimed at reducing the discrepancies in tobacco regulation among Member States. The EU also promotes healthy lifestyles, such as with the HealthyLifeStyle4All campaign. Part of this initiative is the due introduction of an EU mobile app for cancer prevention to aid the novel cancer plan.
In 2021, the European Commission presented the Europe’s Beating Cancer plan. This entails a complex variety of initiatives to decrease the cancer burden in the EU. Most notably, the Commission will push cancer-screening across Europe to enhance early diagnosis. Preventive measures are accentuated by the proposal to vaccinate 90% of girls and a substantial number of boys against human papillomavirus (HPV) while patient care is facilitated through a ‘Cancer Survivor Smart-Card’, which provides patient history and monitors follow-up care. Many of the Cancer Plan’s initiatives have yet to be solidified as it was only recently adopted.
Key Questions
- What can be done for those with rare cancers which have little to no treatment available?
- How will the EBDP ensure patient data privacy? Should any leniency be shown for cancer studies or should patients have full control?
- Is a future free from cancer possible?
- Should the financial burden from foreign patients be placed upon their own insurance or on the host nation?
- Should a focus be placed on the mobility of patients rather than the availability of treatment when pertaining to shortages in personnel or drugs?
Further Reading
- An article on cancer itself, 2019, ABC News.
- The Europe’s Beating Cancer Plan, 2021, European Commission.
- A report on so-called cancer inequality, 2017, Euractiv.
- A comprehensive paper on social-economic status and cancer, 2019, Salvatore Vaccarella et al., editors.