
Committee on Environment, Public Health and Food Safety (ENVI II)
Girls just wanna have fun-damental rights: Women are chronically underrepresented and under-researched in medicine, which often leads to misdiagnosis and dismissal when they seek medical treatment. Given this gender data gap, how can the EU ensure its female population (51%) receives effective treatment?
Chairperson: Maria Cuder
Introduction and Relevance to the topic
Different studies have shown the persistent stereotype that STEMM (Science, Technology, Engineering, Mathematics and Medicine) professionals are white men. Nonetheless, this conundrum does not only affect the society’s expectation of a doctor being a man, but it has affected women’s health in two ways with major implications: firstly, in a lack of research about the female bodies (in comparison with the male one), and secondly, in a dismissal and misdiagnosis when they seek medical treatment. For instance, less than 2.5% of publicly funded research has been dedicated exclusively to female reproductive health, in spite of the fact that 1 in every 3 women will experience severe reproductive health issues in their life.
On social media, women like Paige Layle on TikTok have given voice to the difficulties that women face in diagnosis, in her case, autism. This is due to the fact that when doctors study autism, they tend to focus on men, that is why men are normally diagnosed in the first years of their lives while women learn to “mask”1Mask: hiding their traits and adopting the behaviors of people around them who do not live with autism.. In addition, Layle mentions how people assumed she does not have the disorder as women tend to have different symptoms that are not as known as the “regular” symptoms of autism that men show.
Nonetheless, this issue is not only affecting some late diagnosis, but also, can lead to a point where women could have a chance of dying because of these situations. Some women´s medical issues are being dismissed by the fact that their symptoms are different than the ones males show. For example, the case of a woman in her 40s, who is diagnosed with anxiety, when in reality, she was having a heart attack. She was told to have no symptoms,when in reality, she did, just not the typical “male” ones.
Key Conflicts
Lack of representation
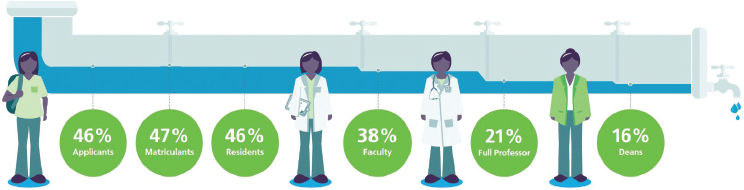
In academic medicine, where in 2018 for the first time the number of women exceeded the number of men, there is still an underrepresentation at senior academia or leadership positions that cannot be explained by the time lag between finishing their degree and starting their career trajectory.
More than a decade ago, women achieved parity with men in the number of matriculants in medical schools. Nonetheless, there are still differences in pay, academic ranks and leadership positions for women compared to men in academic positions. It is true that the situation is improving, nonetheless, the progress is slow.
Issues in research
Given that history was dictated by men, it is easy to understand that the background behind this issue lies in the fact that women have had a sense of being “othered” in the human species, which has highly affected their health. This has led society to the point that, in the present, there has been 5 more times research into male erectile dysfunction (affects a 19% of men), than there has been into premenstrual syndrome (which affects a 90% of women).
Misdiagnosis
A study by the British Heart Foundation (BHF), showed that women who suffer heart attacks are only half as likely as men to receive the recommended treatment. This can be followed by another research by the BHF, which revealed that 8000 women in England and Wales had died of misdiagnosed or untreated heart attacks that they had tried to report (over a 10-year period).
In general, a study has proved that women are diagnosed years later than men for the same disease. Researchers do not know if the later diagnoses are due to genetics, the environment or possible biases in the healthcare system (or a combination of everything). Nonetheless, the issue is there. On average, women received cancer diagnoses 2.5 years after men, and metabolic diseases diagnosis (e.g. diabetes), 4.5 years later.
Furthermore, not only are women diagnosed later, but also, they are misdiagnosed at an alarming rate compared to men. For example, women are 30% more likely to have symptoms of a stroke misdiagnosis and be, erroneously, sent home from the emergency room.
Wrong doses given to women
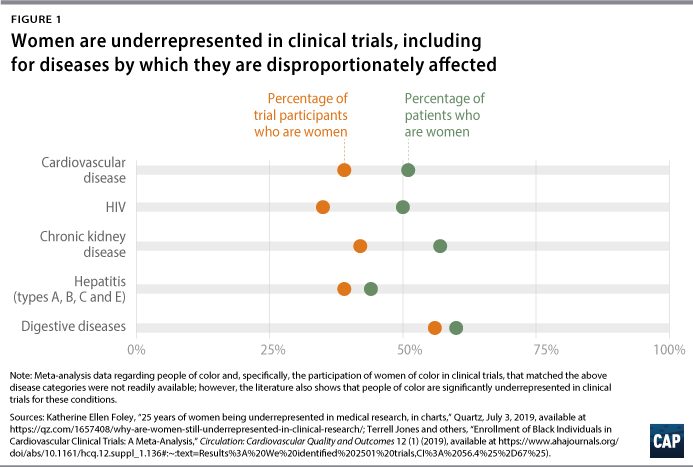
Some medicines affect women and men differently, which sometimes leads to women receiving excessive doses of drugs. On one hand, the difference between men and women’s bodies is not usually considered (weight, percentage of body fat, hormones etc.). So women and men are given the same dose based on a one-size-fits all dosage, which eventually means that, on average, women are being overdosed on most drugs. On the other hand, the wrong dose is produced by the exclusion of women in certain studies in order to simplify the trials by assuming the men’s body responses stay the same for women. Besides, the fact that, depending on where the woman is in her menstrual cycle, the variation of hormones “complicates” results, leads to some studies leaving women out in the experiments and trials.
Between the consequences of these actions, it can be highlighted that eight out of ten drugs removed from the markets in the United States between 1997 and 2000 were withdrawn because of their side effects affecting mainly or exclusively women. In addition, between 2004 and 2013, American women had more than 2 million drug adverse events, in comparison to 1.3 million for men.
Dismissal when asking for help
Nevertheless, this is not the only way female bodies are put at risk, it also happens when women are dismissed when they ask for treatment as a consequence of the stereotype of women complaining more than men. The gender gap is fed by stereotypes of women being over-emotional and how they exaggerate the level of pain and suffering. However, in reality, it is proved that many women under-report symptoms, and not being taken seriously when asking for a medical treatment, can propagate the notion that what they have is not important, which can have health consequences.
Key Actors
World Health Organisation (WHO): its primary role is to direct international health within the United Nations system and to lead partners in global health responses.
European Institute for Gender Equality (EIGE): a European agency that works to promote and ensure equal opportunities for women and men across Europe and beyond through quality evidence for better policy making. It delivers high quality research and information to support European institutions and countries in their efforts to end gender inequalities.
European Medicines Agency (EMA): its main responsibilities are authorising and monitoring medicines in the EU. Companies apply to it for a single market authorisation, which is issued by the European Commission. If granted, this enables them to market the concerned medicine throughout the EU and the EEA. Given the wide-ranging scope of the centralised procedure, most genuinely innovative medicines marketed in Europe are authorised by the EMA.
European Institute of Women’s Health (EIWH): a non-governmental organisation (NGO) that promotes gender equity in public health, research and social policies across Europe.
Measures in Place
In the strategy on women’s health and well-being in the WHO European Region (2016), measures to be taken by the Members States can be found. Their aim is:
- Strengthening governance for women’s health and well-being, with women at the center
- Eliminating discriminatory values, norms and practices that affect the health and well-being of girls and women
- Tackling the impact of gender and social, economic, cultural and environmental determinants on women’s health and well-being
- Improving health system responses to women’s health and well-being
The European Commission has recently agreed on a 25 million euro strategic partnership with the World Health Organisation, which includes support to strengthen problems for maternal and child health. They both are committed to work together to accelerate the progress on reducing maternal, neonatal and child mortality.
Governments like the UK have committed to tackle the gender gap in medicine by dismantling barriers, making senior roles more accessible to women, improving pay transparency and promoting cultural change.
The EUGenMed (European Gender Medicine) have different projects and are taking different approaches to this issue, all of them can be found on their page and are related to current issues. For instance: doing a research project on the impact of the health crisis caused by COVID-19 on gender inequalities in Portugal.
The World Health Organisation (WHO) has a report from 2017 on how gender equality is necessary to make everyone healthier. In this report, the consideration of future measures to help women is talked about, for example, the need to empower women with negotiation skills in China so smoke-free homes are created that benefit entire families.
Questions to think about
- How can the EU ensure that there is an increase in the research of the female body?
- How can the EU address the fact that women are being put at risk after dismissal or misdiagnosis?
- Which measures can the EU take so that there are enough women represented in academic medicine?
- Which steps can the EU take so that women receive a right dose of drugs?
Links for further research
- Lack of females in drug dose trials leads to overmedicated women | Berkeley News
- Why Are Women Dying When They Reach Hospital on Time? A Systematic Review of the ‘Third Delay’ (plos.org)
- Compensation and Advancement of Women in Academic Medicine: Is There Equity? | Annals of Internal Medicine (acpjournals.org)
- Misdiagnosis and the Gender Gap (armadahealth.com)
- Video:Misdiagnosis: The battle for the female body in a man-made world • FRANCE 24 English – Bing video (women in science in general)
Introductory Clauses
The European Youth Parliament,
- Concerned by the frequent misdiagnosis when women seek medical treatment in comparison to men,
- Noting with regret the lack of research in relation to the women bodies as a consequence of using the male bodies in order for these studies as a way to “simplify them”,
- Bearing in mind that women are underrepresented in higher academic roles,
- Aware that women are sometimes given the wrong drug dosage as a consequence of setting the male body as a standard,
- Fully alarmed by the fact that female health issues are sometimes not given enough importance because of the stigmatisation of women as “complaining”,
- Acknowledging the fact that, women often receive their medical diagnoses later than men,
